


'We need our MPs to act now.'

On 26 February 2026, Members of Parliament and the House of Lords gathered at an event in Parliament sponsored by Richard Burgon to launch a new working paper and discuss growing concerns about NHS privatisation. The panel included experts from Keep Our NHS Public, the Nuffield Trust, and the 99% Organisation. The discussion addressed three central questions: What counts as healthcare privatisation? How much is really taking place? And does it matter, particularly for patients?
The debate often begins with denial. Successive governments have claimed that the NHS is not being privatised and never will be. Some rely on the phrasing that the NHS is not “for sale,” while others stress that it remains “free at the point of use.” The World Health Organization (WHO) defines privatisation as any process that increases private sector involvement in the financing or delivery of healthcare. This definition captures changes that political slogans do not.
Imagine if the NHS were gradually reduced to a small share of overall healthcare provision through underfunding—while remaining technically free at the point of use—it could still meet political definitions of being “not for sale,” yet the UK’s universal healthcare system would have disappeared. Under the WHO’s definition, such a shift would clearly constitute privatisation. The panel argued this broader definition is both more honest and more illuminating.
There are at least five routes through which privatisation can occur. The most common is contracting out: NHS-funded services delivered by private companies. Second, patients may be squeezed out or even thrown out if services are rationed, withdrawn, or subject to new charges, forcing people into private payment. Third, the Private Finance Initiative (PFI) replaces public borrowing with more expensive private finance. Fourth, private firms can gain influence through governance or management roles within the NHS. Finally, assets or services may be directly sold off, though this is less common.
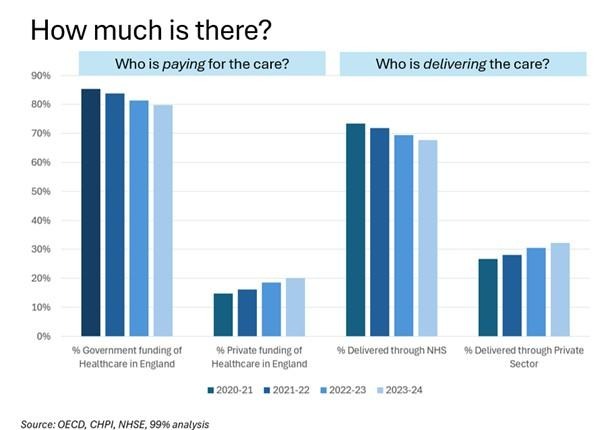
Public discussion frequently cites a figure of around 7% to suggest privatisation is minimal and stable. However, this figure captures only a narrow slice of contracting-out and ignores the growing share of care paid for privately by patients. Once those omissions are corrected, the picture changes substantially.
{kind=link}
Around 20% of UK healthcare is now paid for privately, either out of pocket or via insurance. When adding NHS-funded services delivered by private providers, over 30% of healthcare delivery is now in private hands, with some specialties exceeding 50%. Far from being marginal, private sector involvement is significant and expanding.
The most critical issue is whether this shift affects patients.
Ophthalmology, particularly cataract surgery, illustrates the concern with contracting out. Simple cataract operations can be performed quickly and profitably, and private “cataract factories” specialise in high-volume delivery. While this may reduce waiting lists, it distorts clinical priorities. Early removal of mild cataracts offers limited medical benefit, while conditions such as glaucoma or macular degeneration require urgent treatment to prevent irreversible blindness. The president of the Royal College of Ophthalmologists described the result of the extensive use of cataract factories as patients with very mild cataracts “getting surgery at the expense of other patients going blind.”
The patient receiving swift surgery may be satisfied, but the patient who goes blind would be horrified.
Dentistry offers another example. Although NHS dentistry remains available in theory, many areas have become “dental deserts” where NHS appointments are nearly impossible to secure in practice. Some treatments have largely disappeared from NHS provision. Patients are effectively squeezed out into private care or left untreated. The poorest are hardest hit, and the British Dental Association reports widespread cases of attempted do-it-yourself dentistry. Here, privatisation does not expand choice; it restricts access.
Joint replacements reveal a similar pattern. While some patients choose private treatment to avoid long waits, others are thrown out of the NHS altogether. Despite guidance from NICE that obesity should not automatically block referral, many Clinical Commissioning Groups have applied body mass index thresholds that deny treatment. Patients who cannot access NHS care may have no realistic alternative. In these cases, privatisation is not about preference but exclusion.
Private finance has imposed long-term costs on public finances. Governments have sometimes used PFI to avoid the appearance of public borrowing. The theory was that bundling construction, financing, and management would deliver efficiencies offsetting higher financing costs. In practice, as the National Audit Office concluded, PFI schemes have delivered poor value for money.
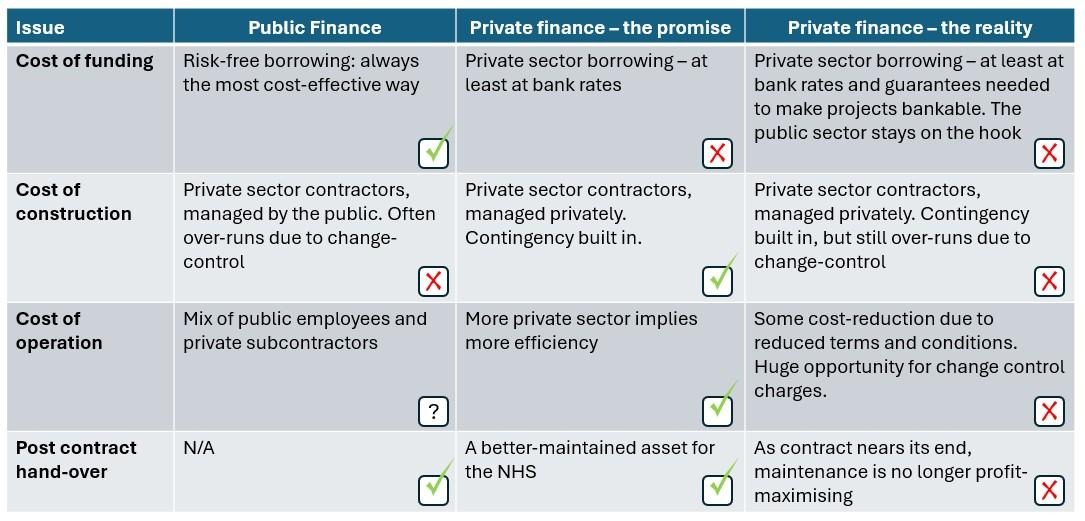
The public sector can borrow more cheaply, and promised efficiencies often failed to materialise. As a result, NHS budgets have been burdened with expensive long-term repayment commitments.
Governance presents further challenges. Private companies are legally required to prioritise shareholder returns. Under company law, directors must put profit first. This obligation often conflicts with the NHS’s mission to maximise patient care and value for taxpayers. Corporate providers must focus on profitable services, patients, and regions. When profits fall, they withdraw provision. In 2015, Circle Health exited management of Hinchingbrooke Hospital, citing financial viability concerns. In 2023, Centene withdrew from providing GP services in London when profits proved insufficient. Such exits leave gaps that the NHS must fill, or else services deteriorate.
The panel concluded that three common claims about privatisation are misleading: that it is not happening, that it is minimal, and that patients benefit from it. Evidence suggests privatisation is significant and increasing; its effects include distorted clinical priorities, exclusion of vulnerable patients, higher long-term costs, and governance conflicts. We urged Policymakers to recognise that current trends risk undermining patient care, straining public finances, and eroding the foundational principles of the NHS itself. We need our MPs to act now.
Mark E Thomas, Founder of the 99% Organisation
Image credit: Garry Knight – Creative Commons
Left Foot Forward doesn't have the backing of big business or billionaires. We rely on the kind and generous support of ordinary people like you.
You can support hard-hitting journalism that holds the right to account, provides a forum for debate among progressives, and covers the stories the rest of the media ignore. Donate today.